
Who Decides When a Woman Has a Child?
By: Melanie MacEachern and Paula Blankenship with additional reporting from Christopher Dorch
Arizona’s position on a women’s right to bodily autonomy started before Arizona’s own birth as a state in 1912. The territorial revised statutes from 1901 made it illegal for anyone to assist a pregnant woman to miscarry unless to preserve the mother’s life.
More than a century later, Arizona’s Republican majority passed Senate Bill 1164, currently an abortion restriction with echoes of Arizona’s territorial past when laws denied women the right to vote and forced women to carry to term unwanted pregnancies.
Passed by the Arizona Legislature March 24 and signed into law March 30, SB 1164 bans fully licensed medical providers from performing an abortion beyond 15 weeks of gestation and offers no exception for rape or incest. Arizona’s new abortion law hinges on this summer’s abortion ruling from the U.S. Supreme Court which could weaken or overturn Roe v Wade, the high court’s 1973 decision that largely made state abortion bans symbolic because it sealed the right to abortion for all American women.
Madeline Eells, MD, an obstetrics and gynecology specialist in Tuba City, is a traveling abortion provider at Planned Parenthood in Flagstaff. She feels the effects of Arizona laws restricting abortion every time she encounters a pregnant patient.
Many times I feel like I cannot adequately provide patient care due to the presence or the impending presence of legislation in my clinic room. It should be you and the patient.
Eells never offers congratulations to a patient on her pregnancy because “I don’t know where she’s at.” But once the pregnancy is confirmed she reminds patients that every pregnancy can end in one of three ways.
- Continue the pregnancy with the intention to parent
- Continue the pregnancy with the intention to adopt
- End the pregnancy, otherwise known as abortion
Arizona’s Newest Abortion Ban
The Arizona legislation directly mirrors the 2018 Mississippi abortion ban currently under consideration by the U.S. Supreme Court (SCOTUS) and targets physicians who knowingly perform an abortion after 15 weeks.
A physician who performs an abortion in Arizona after 15-weeks, outside a medical emergency, will lose their medical license. Other penalties include a Class 6 felony – an offense akin to sexual conduct with a minor, resisting arrest and aggravated domestic violence. Physicians who falsely report or fail to report an abortion outside the legal limit are subject to a civil penalty of $10,000.
Physicians and pregnant women in Arizona now live and work in one of the few states with an abortion ban still standing from an era before Roe v. Wade. An expected summer ruling from SCOTUS supporting the Mississippi law will significantly impact abortion care for a new generation of American women.
American obstetricians and gynecologists have already made their case for protecting women’s right to abortion.
American College of Obstetrics and Gynecologists (ACOG),
Induced abortion is an essential component of women’s health care. Like all medical matters, decisions regarding abortion should be made by patients in consultation with their healthcare providers and without undue interference by outside parties.
The Supreme Court has until June to mull over oral arguments presented last November on Dodd v. Jackson Women’s Health, a case concerning the legality of a Mississippi 15-week abortion ban. Roe’s demise has rarely seemed so imminent, except in 1992, when the Republican dominated Rehnquist Court constructed a Gordian knot of jurisprudence, both upholding and undermining legal abortion with the ruling in Planned Parenthood of Southeastern Pennsylvania v. Casey.
The Casey decision dismantled the trimester framework of gestational development upon which the Roe decision hinged, shifting instead to viability, or the ability for a fetus to survive outside the uterus. In the Roe v Wade decision Justice Harry Blackmun established the trimester structure to roughly estimate fetal development.
Cornell Law School summed up the structure set forth by SCOTUS,
First Trimester
Decision to terminate the pregnancy was solely at the discretion of the woman, but the state could “regulate procedure.”
Second Trimester
The state could regulate (but not outlaw) abortions in the interests of the mother’s health.
After the Second Trimester
Fetus became viable, and the state could regulate or outlaw abortions in the interest of the potential life except when necessary to preserve the life or health of the mother.
A former Arizona legislator would play a pivotal role in the rejection of Blackmun’s approach.

Courtesy of The New Yorker
Justice Sandra Day O’Connor, the first woman appointed to the Supreme Court and a former Arizona legislator, expressed disapproval of the trimester framework. Lamenting the arbitrary nature of a non-scientific justification applied to juridical rulemaking, she said it put the Court in the wrong business.
Justice Sandra Day O’Connor,
There is simply no justification in Constitutional theory for having a different standard or test for the different trimesters. Seems it puts us in the business of being a science review board.
In her personal notes during the Reagan era, Justice O’Connor also wrote,
I would permit state regulations at every stage which do not unduly burden the right of the woman to terminate her pregnancy.
Even so, Justice O’Connor, along with Justices Anthony Kennedy and David Souter, threw out the trimester framework for the establishment of the “undue burden,” which provided a juridical – rather than scientific point at which the state could interfere with a woman’s choice to have an abortion.
“Though the woman has a right to choose to terminate or continue her pregnancy before viability, it does not at all follow that the State is prohibited from taking steps to ensure that this choice is thoughtful and informed,” the plurality Casey opinion read.
There is no other line than viability which is more workable.
This decision arguably had more effect on the state of abortion services in the United States than even Roe v. Wade. Casey freed states to regulate abortion as they deemed necessary, with or without advice from the medical community.
Anti-abortion groups used the Casey decision to justify and lobby for ever-increasing constraints on providers, requirements for patients, interventions from third parties in patient care, all in pursuit of regulating abortion and its providers out of existence.
Proponents of women’s right to choose were soon referring to such policies as targeted restriction of abortion provider (TRAP) laws because they place medically unnecessary requirements on clinics and providers to force them to stop providing abortion care. Inspired by the ambiguous framework set forth in the Casey decision, TRAP laws attempt to place burdensome regulations on abortion providers
In 2011, the American Medical Association Journal of Ethics characterized TRAP laws as representing an unprecedented level of intrusiveness in the doctor-patient relationship. They described it as a thorough disregard for the exercise of independent medical judgment,
Regardless of beliefs concerning abortion, all physicians have reason to object on professional grounds to state interference with the practice of medicine.
The American College of Obstetrics and Gynecology put it even more succinctly,
The best healthcare is provided free of political interference in the patient-physician relationship.
For decades, mostly Republican legislators in Arizona have disagreed. Since 2000 more than 50 restrictions on abortion, abortion providers and reproductive healthcare clinics have been up for consideration. Fourteen became law, including
- Criminalization of later term abortion procedures
- Ban on telemedicine services to acquire abortion pills
- 24-hour mandatory waiting period for an abortion
- Qualified nurse practitioners, certified nurse midwives and physician assistants are barred from providing an abortion
Stand out TRAP laws include Arizona’s 2012 “Women’s Right to Know Act” and 2015’s SB 1318 requiring abortion providers to tell women receiving medication-induced abortions that the procedure can be reversed, even though medical professionals tell us it can’t.
According to The American Congress of Obstetricians and Gynecologists there is no medically accepted evidence that a drug-induced abortion can be interrupted.
Claims of medication abortion reversal are not supported by the body of scientific evidence, and this approach is not recommended in ACOG’s clinical guidance on medication abortion.
Facts and scientific evidence haven’t stopped Arizona legislators from pursuing increasingly restrictive policies that create barriers to abortion in the state. The Guttmacher Institute, a frequent collaborator of The World Health Organization, has kept track.
Arizona Abortion Restrictions
Flip Me
Arizona Abortion Restrictions
- A patient must receive state-directed counseling that includes information designed to discourage the patient from having an abortion, and then wait 24 hours before the procedure is provided. Counseling must be provided in person and must take place before the waiting period begins, thereby necessitating two trips to the facility.
- Health plans offered in the state’s health exchange under the Affordable Care Act can only cover abortion in cases of life endangerment or severely compromised physical health.
- Abortion is covered in insurance policies for public employees only in cases of life endangerment or severely compromised health.
- The use of telemedicine to administer medication abortion is prohibited.
- The parent of a minor must consent before an abortion is provided.
- The Medicaid program does not provide coverage for medically necessary abortions, despite a court order directing it to do so.
- A patient must undergo an ultrasound at least 24 hours before obtaining an abortion; the provider must offer the patient the option to view the image.
- An abortion may be performed at or after viability only if the patient’s life or health is endangered.
- The state prohibits abortions performed for the purpose of race or sex selection.
The state requires abortion clinics to meet unnecessary and burdensome standards related to their physical plant, equipment and staffing
At the beginning of the pandemic, Republican Governor Doug Ducey expanded the use of telemedicine services for anything covered by insurance for an in-person visit, except for abortion. The governor’s March 25, 2020 executive order did not supersede a 2011 law explicitly banning the use of telemedicine for any abortion procedure.
Arizona is one of six states in the nation with a telemedicine restriction that defies science and ignores a major determinant of overall good health: access to providers.
With a population of 3 million women, Arizona has only nine licensed abortion clinics. In 2021, after extensive scientific review, the FDA scrapped its in-person requirement for Mifepristone, a medication that is used in combination with another drug, Misoprostol, to end a pregnancy.
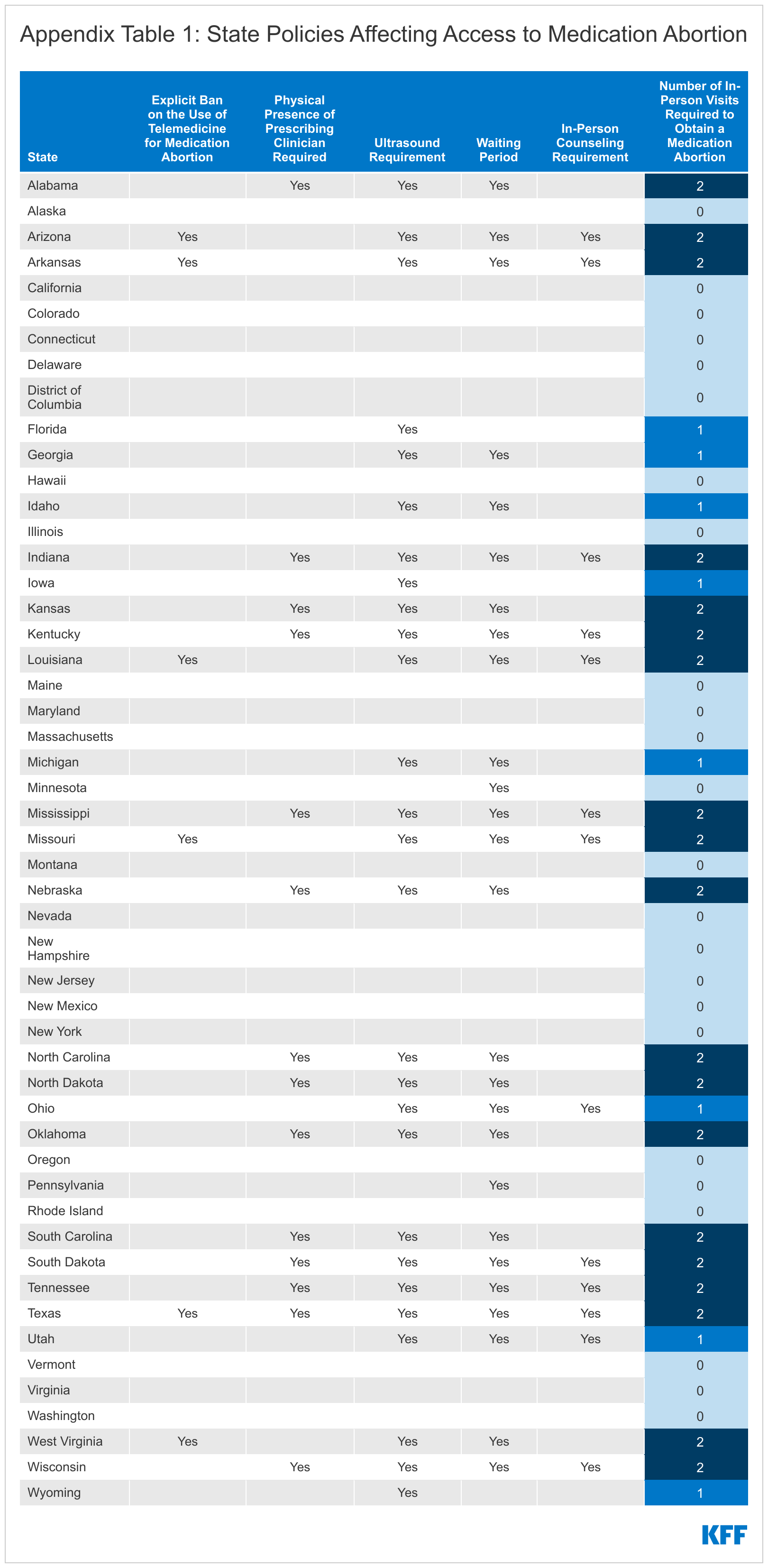
Kaiser Family Foundation
From the Kaiser Family Foundation,
The FDA has never required Misoprostol to be dispensed by a doctor or taken at a medical facility and there is no FDA requirement for an in-person follow-up visit.
Telemedicine Restrictions on Abortion Pill
 The expansion of telemedicine allowances in Arizona since the COVID-19 pandemic has shown an increased ability for providers to connect with rural patients. However, restrictions on the administration of prescription of the abortion pill means patients must travel to a city with an abortion provider and stay overnight to fulfill the 24-hour waiting period requirement.
The expansion of telemedicine allowances in Arizona since the COVID-19 pandemic has shown an increased ability for providers to connect with rural patients. However, restrictions on the administration of prescription of the abortion pill means patients must travel to a city with an abortion provider and stay overnight to fulfill the 24-hour waiting period requirement.
Most abortion patients are poor or low income, and many also pay out of pocket for abortion care, according to the Guttmacher Institute,
When all abortion care must be administered by a physician, it can be prohibitively expensive for poor patients.
Not only is the cost of abortion expensive at an average of $650 for the abortion pill and surgical procedures, it also requires the patient to pay for overnight amenities and take time off work. Factor in gas and other travel expenses, and poor, rural, Arizona women are faced with over $1,000 in expenses.
Dr. Eells, the traveling OB/GYN who serves northern Arizona communities and provides abortion services at the Planned Parenthood Flagstaff location, explained how this impacts her patients.
I might encounter a patient in my normal practice who is on the reservation and communicates to me that she wants counseling about the full scope of her pregnancy options. Then, I have to make clear to them that they need to plan time not only to locate the resources, take time off of work, plan the financial resources to have a consultation at one of the Planned Parenthood facilities or one of the private facilities that offer abortion counseling services in the state of Arizona, but then they have to, if they’re lucky, make an appointment exactly 24 hours later.
She also explained how the waiting period conflicts with a patient’s ability to receive medical abortion before the cutoff date of 12 weeks.
So now, they not only have to wait that 24-hour period, but now they’re coming down to Phoenix in order to seek out a surgical or in-clinic abortion procedure.
These difficulties extend to teenagers, who are required to obtain notarized written permission from a parent or legal guardian, or permission from a judge. The National Abortion Federation estimates that restrictive abortion laws inhibit teenagers from seeking medical care early in their pregnancies:
When teens know that healthcare providers are forced by law to tell their parents before providing services, they are less willing to get care related to sexual activity.
There are also directly obtrusive measures that interfere with a provider’s ability to deliver medical care to patients in a manner informed by medical consensus.
Doctors Supporting Current US Abortion Law
Doctors Against Restricted Access to Comprehensive Reproductive Healthcare
American Academy of Family Physicians
American Academy of Nursing
American Academy of Pediatricians
American Association of Public Health Physicians
American College of Medical Genetics and Genomics
American College of Nurse-Midwives
American College of Osteopathic, Obstetricians and Gynecologists
American Medical Women’s Association
American Psychiatric Association
American Society for Reproductive Medicine
Association of Women’s Health, Obstetric and Neonatal Nurses
American Medical Association
National Association of Nurse Practitioners in Women’s Health
Society for Academic Specialists in General Obstetrics and Gynecology
Society of OB/GYN Hospitalists
American College of Obstetricians and Gynecologists
The Born Alive Debate
In 2017, Governor Ducey signed SB 1367, which requires attending physicians “see that all available means and medical skills are used to promote, preserve and maintain the life of [a] fetus or embryo.” Under the law, all clinics are to maintain a staff member designated to deliver “a fetus delivered alive” to a hospital and a staff member trained in neonatal resuscitation.
There are very few situations in which a fetus is born alive during an abortion and almost all occur in abortions induced to save the life of the mother. For example, a condition called pre-eclampsia can kill both the mother and the fetus, and the recommended treatment is to deliver the baby. In cases where the fetus will not survive, families often elect to provide comfort care and allow the infant to die naturally.
Comfort measures are interrupted in Arizona, when physicians must perform an examination to confirm a fetus’ lethal condition after birth. In his letter opposing the legislation, Neonatologist Dr. Peter Stevenson wrote the decision to resuscitate depends on whether intervention is futile. Fetuses born at 20 to 21 weeks gestation have zero chance of survival and the standard of care nationwide is to provide “comfort measures” instead of resuscitation, he wrote in a letter to the Legislature, reported by The Arizona Republic.
The law requires doctors to take measures to “maintain the life” of any fetus delivered alive during an abortion – regardless of gestational age. According to AZDHS, of the 13,186 Arizona abortions in 2020, nine abortions involved a fetus or embryo delivered alive in Arizona.
Some Arizona state legislators, like Senator Juan Mendez (D-Tempe), former Senator Andrew Sherwood (D-Tucson) and Secretary of State Katie Hobbs have attempted to repeal these TRAP laws through legislation on the advice of healthcare providers and medical institutions. Of the 26 proposed bills in the past decade, none have progressed out of committee.
Title X Restrictions
Restrictions on Title X Funding have also been effective in limiting access to abortion in Arizona. In 2017, the Trump administration Department of Health and Human Services reimplemented a Reagan-era rule that barred health centers from receiving Title X funding if they counseled patients on pregnancy options that include abortion, referring patients to an abortion provider, or offering abortion as a method of family planning. Title X funding is a federal service grant program that assists low-income individuals and families with reproductive and sexual health care services for the purpose of family planning.
Arizona’s Title X funding is administered through the Arizona Family Health Partnership, a 501(c)(3) that distributes the grant funding to participating providers including mobile care units, urgent care providers, clinical care practices and federally qualified health centers.
According to a 2018 report to the U.S. Senate Health, Education, Labor and Pensions Committee, Planned Parenthood Arizona represented 17% of total sites associated with the funding but accounted for more than half of the grant’s total patients. It was estimated that the impact of redirecting funds would require Federally Qualified Health Centers (FQHCs) to increase their caseloads by 90% to reach the number of patients served by Planned Parenthood. As a result, between 2018 and 2020, the number of Title X female contraceptive patients fell 60%, from 29,319 to 12,287. The harm caused is quantifiable – over 15,000 fewer people received contraception in a two-year period in Arizona due to concerns about money getting too close to abortion to be considered comfortable for legislators.
Hoping to force Planned Parenthood off the Title X network, the Arizona State Legislature passed SB 1527 in 2017, which required the Arizona Department of Health Services to apply for the Title X grant. ADHS does not provide family planning services or direct patient care. According to the Guttmacher Institute, the agency was awarded 25% of the state’s Title X funding, limiting the Arizona Family Health Partnership to only 75% of its usual award.
Initially, the plan didn’t work, but in 2019 the Trump Administration released a final rule barring clinics that provide or refer patients for abortions from receiving federal family planning funds. Planned Parenthood Arizona voluntarily left the partnership to continue providing abortion care at its clinics.
Preventing Unwanted Pregnancy
If Arizona wants fewer abortions, research concludes the first step is through family planning services, education, and the wide availability of contraceptives.
The Centers for Disease Control has a list of the things it’s working on to prevent unintended pregnancy. Not on the list: less access to family planning services.
CDC Tips for Preventing Unwanted Pregnancy
CDC's Approach to Preventing Unintended Pregnancy
- Examine the need for contraceptive services among women of reproductive age.
- Increase access, use, and dissemination of data to identify groups most at risk for unintended pregnancy; show the health impacts of teen and unintended pregnancy; and close gaps in access to quality, patient-centered family planning services.
- Develop and identify evidence-based strategies to reduce unmet needs for quality family planning services among the most affected groups.
- Provide guidance for health care providers who counsel men, women, and couples about contraception.
- Build capacity for health care providers, states, communities, and partners to improve quality patient-centered family planning services and support states and communities to increase access to contraception services.
The Arizona State Legislature has showed a good faith effort to closing the gap on preventative care, at least in terms of the delivery of self-administered contraceptives including oral birth control pills, hormonal contraceptive vaginal rings and hormonal patches. In June 2021, Governor Ducey signed SB 1082, legalizing retail, over-the-counter oral contraceptives for qualified patients 18 and older. The legislation also instructs the Arizona State Board of Pharmacy and the Arizona Department of Health Services to adopt rules for the law to go into effect; neither have publicly addressed or released rules to accompany the law, making it impotent.
Several of the Legislature’s most anti-abortion legislators voted against the bill, linking contraceptives to abortion inducing drugs.
In 2019, data from the Guttmacher Institute, the only research organization that strives to count all abortions in the U.S., making inquiries of individual providers, suggests that the 14% decline in abortion rates in the U.S. from 2017 to 2018 was largely due to the increase in availability of oral contraceptives, access to reproductive healthcare and education initiatives. The Affordable Care Act requires most private health insurance plans to cover contraceptives with no out of pocket cost.
The Arizona Health Care Cost Containment System (AHCCCS), Arizona’s Medicaid program, does not provide coverage for medically necessary abortions. Half of all babies born in Arizona are on Medicaid.
Where Are The OB-GYNs in Arizona?
Lack of abortion access means more unwanted babies and more live births, which in Arizona translates to an additional burden on Arizona’s Medicaid program and rural women who can’t locate an OB-GYN to ensure their health and the health of their baby throughout pregnancy and birth.
Analysis from a 2021 assessment of Arizona’s primary care needs by the Bureau of Women’s and Children’s Health at the Arizona Department of Health Services (ADHS) directly links disparities in maternal and birth outcomes by rurality with the ratio of OB-GYN providers to the population in rural and urban areas.
In Arizona, Indigenous women in the northern and eastern parts of the state have very limited access to reproductive care. There are about half as many OB-GYNs in rural areas per 10,000 as there are in Phoenix and Tucson. La Paz and Greenlee counties both have no maternal care, meaning that there are no hospitals or providers for obstetric care. Women in Gila, Graham, Cochise, and Santa Cruz counties have fewer than two hospitals and 60 obstetric providers per 10,000 births.
In a report published last year, HHS provided its projection of supply and demand for women’s health service providers and projects Arizona will meet only 70% of demand for OB-GYNs by 2030.
From Institute of Medicine (US). Science and Babies: Private Decisions, Public Dilemmas,
Many women in the United States do not receive sufficient care: those who are still in their teens; who are black, Hispanic, or American Indian; who are unmarried; who are recent immigrants; who have less than a high school education; and who live in poverty. Each year at least 1.3 million women receive insufficient prenatal care, and many of them are the women who most need it.
Instances of infant mortality, low birthrate and late prenatal care are all higher in rural Arizona.
According to the University of Arizona Center for Rural Health, there are just over two OB-GYNs for every 10,000 births in Phoenix and Tucson. In small rural towns, this rate cuts in half, where there is only one OB-GYN physician per 10,000 births.
Even with the elevated doctor-patient ratio in Arizona’s cities, OB-GYNs in Phoenix are also reporting a higher workload than the national average. According to a 2018 study by Doximity, America’s largest professional medical network, Phoenix OB-GYNs have the fourth highest workload in the county, with 135 births per year per provider. The study notes that shortages of OB-GYNs are directly related to increasing workload demands for the delivery of reproductive healthcare services.
A subsequent Doximity 2019 study found that Phoenix ranks 14th in the country for lowest percentage of OB-GYNs younger than 40. The COVID-19 pandemic highlighted the urgency of building an adequate workforce of younger providers to replace an aging and retiring workforce. Unfortunately, Arizona’s rate of retention of doctors after residency is 55% according to The Association of American Medical Colleges.
“We face real challenges in recruiting and retaining physicians in Arizona. We are training more physicians in our medical schools than we are actually retaining in residency,” said Jennifer Carusetta,
Executive Director of Health Systems Alliance of Arizona.
As medical students research their residency programs, some may be deterred by the strict requirements Arizona places on OB-GYN students. This, in addition to the relatively small number of available OB-GYN residency positions, puts a squeeze on this specialty dedicated to women’s health. In 2022, just over 20 OB-GYN residencies were matched in Arizona.
Dr. Eells took measure of Arizona’s abortion decision during her research for a residency program and made a point of ranking higher those that “valued complex family planning.” She explained,
Complex family planning was important to me when I was interviewing for residency, and I will freely admit that I did not rank [my residency program] even in my top three.
Julie Kwatra, MD a Scottsdale OB-GYN with Arizona Women’s Care and a passionate advocate for reproductive access agreed:
I would assume that there are some people that do not want to practice in a state where they cannot give women the full range of healthcare. And I can tell you, personally, if I were finishing a residency, I would never want to live in Texas. Just on principle, because [Texas anti-abortion legislation] is just so draconian and antithetical to every medical ethic.
As a critical aspect of the full spectrum of reproductive care, criminalizing abortion may serve to alienate the providers that Arizona wants to attract.
Lawyer Timothy Sparling, a legislative advocate with the Arizona Attorneys for Criminal Justice opposed Arizona’s latest abortion restrictions, noting:
It will actually chill good faith operations that doctors would otherwise perform even if this bill had some kind of safe harbor carve out. This bill is basically weaponizing the criminal law to further advance this cultural war over abortion.
Physician Attitudes on Abortion
In a 2021 paper published by the American Public Health Association, physician attitudes about abortion policy’s impacts on patients and the larger practice of medicine and public health are surprisingly under researched and underused.
“Medical and public health leaders have argued against legislative interference with doctor–patient relationships and have underscored physicians’ critical role in shaping healthcare policy. But abortion, a healthcare procedure involved in 25% of all US pregnancies is often omitted from studies of physician attitudes and their potential policy influence.”
Wisconsin abortion restrictions, like those in Arizona include a mandatory 24-hour waiting period, a prohibition of telemedicine for the abortion pill, and a ban on insurance coverage of abortion for state workers and on policies sold through Arizona’s Marketplace.
In 2019, when 1,357 Wisconsin physicians were surveyed, they weren’t on the fence. An overwhelming majority (80%) supported abortion healthcare services and unrestricted access to abortion. More than four in five physicians said they had at least some concern that restrictive abortion laws would make it difficult to recruit faculty.
Protecting Life
When women don’t have access to abortion and are forced by the state to carry their unwanted pregnancy, “protecting life” takes on a different context in the abortion debate.
In 2017, ProPublica and National Public Radio jointly published a groundbreaking research project that definitively demonstrated that the United States has the worst rate of maternal mortality in the developed world. In 2019 alone, more than 754 women died while pregnant or within 42 days after birth, up nearly 100 deaths from 2018. Nationally, Black women account for the largest percentage of these deaths when broken down by race, at rates over twice as high as white women and nearly four times the rate of Hispanic women.
From the study, Health Care Disparity and Pregnancy-Related Mortality in the United States, 2005-2014
The current U.S. maternal mortality ratio is heavily influenced by a higher rate of death among non-Hispanic Black or unmarried patients with unplanned pregnancies. Racial disparities in healthcare availability and access or utilization by underserved populations are important issues faced by states seeking to decrease maternal mortality.
Arizona ranks 40th nationally for maternal mortality, with 22 deaths per 1,000.
Severe maternal morbidity is an even greater concern for pregnant women. Between 2013 and 2014, severe maternal morbidity affected nearly 15 out of every 1,000 deliveries and is characterized by maternal health outcomes related to pregnancy that could lead to death, chronic conditions, and lifelong impairment.
States with the most restrictive anti-abortion measures in the country have the most alarming rates of maternal morbidity including Texas, which has the highest number of maternal mortalities, and Louisiana which has far and away the greatest rate with 58.1 per 100,000 births. Not lagging far behind are Arkansas, Georgia, Missouri, Indiana, South Carolina, and Alabama.
One potential remedy for these crushing rates of maternal death is expanding Medicaid coverage for up to one year following birth. In Arizona, a bill expanding this care to otherwise uninsured mothers recently passed the Senate. While this measure will certainly go great lengths to improve maternal outcomes for women in marginalized demographics, it remains important to see Medicaid coverage expansion to pregnant women and mothers one-year post-birth as just one tool to improve the overall health of Arizona women.
According to the University of Arizona Center for Rural Health, one in four rural women gives birth at a non-local hospital and in some areas, nearly half of rural women must travel 30 minutes or more for maternity care. This prohibitive distance means that some care goes delayed or entirely neglected, leading to premature births and could be a contributing factor in Arizona’s maternal mortality crisis.
But bearing most of the burden of maternal health risks are Black and Indigenous women. Regardless of Medicaid status, many will face the systemic obstacles of medicalized racism.
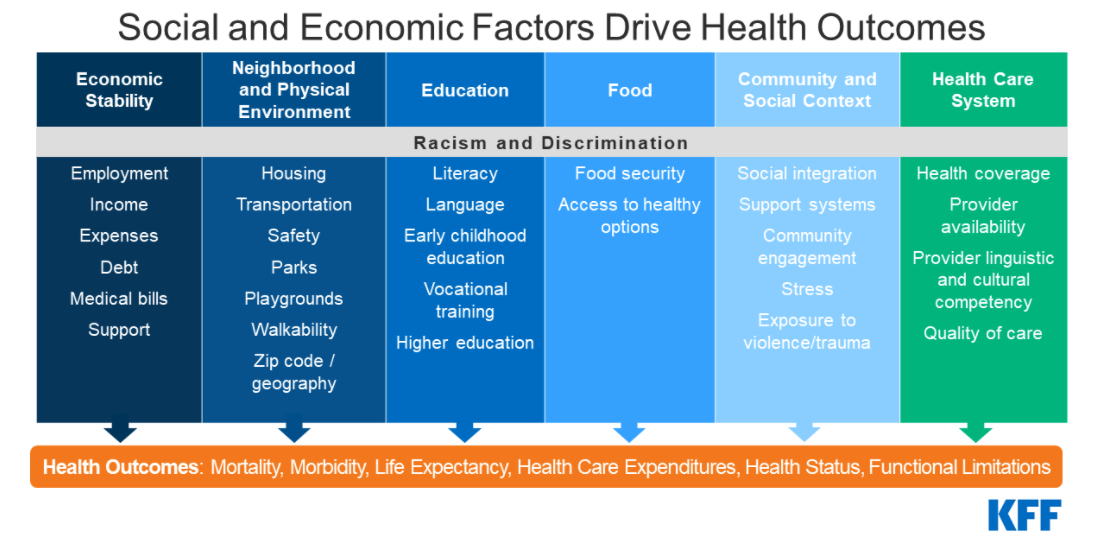
The factors driving disparities in maternal and infant health are complex and multifactorial. They include differences in health insurance coverage and access to care. However, broader social and economic factors and structural and systemic racism and discrimination, also play a major role in shaping health and disparities in health, according to the Kaiser Family Foundation.
Crisis Pregnancy Centers
Although Arizona is short on OB-GYNs, crisis pregnancy centers led by non-clinicians to dispense advice to women facing unplanned pregnancies are easy to find.
Crisis pregnancy centers (CPCs) are organizations that exist to deter pregnant women from seeking abortion. Often, they use ambiguous language and prominent advertising to attract business and frequently have non-clinical employees wear medical scrubs and offer a limited range of non-medical services like over-the-counter pregnancy and STI tests. They are also often found in heavily trafficked areas of college towns, in shopping malls or nearby sexual health clinics.
In 2018, the American Medical Association weighed in on these organizations, and disputed their value:
They strive to appear as sites offering clinical services in unbiased advice. Lay volunteers who are not licensed clinicians at CPCs often wear white coats and see women in exam rooms… Despite looking like legitimate clinics, most CPCs are not licensed, and their staff are not licensed medical professionals. CPCs that are not licensed medical clinics cannot legally be held to the privacy provisions of the Health Insurance Portability and Accountability Act, which could lead to violations of patient privacy.
In 2019, the Center for Arizona Policy supported two mirror bills, HB2579 and SB1547 that would have allocated $7.5 million for a “family health pilot program” for services that would be used to discourage women from seeking or obtaining abortions. The funding would be prohibited from use by any organization that performs or refers for abortion.
In 2021, Senator Nancy Barto introduced SB 1251, a bill that would appropriate $3 million dollars over two years for a “family health pilot program,” which would distribute money to non-profit organizations to “support childbirth as an alternative to abortion” and prohibits the funding from use in referrals for abortion procedures. Although the bill and its mirror in the House, HB2404, both died before reaching a vote, they were included in the year-end Appropriations bill during budget reconciliation.
“I know this all sounds super,” then-Planned Parenthood Arizona vice president of public affairs Jodi Liggett told The Arizona Capitol Times during discussion on the 2019 mirror bills. “But unfortunately, the majority of crisis pregnancy centers are not neutral in their approach to women. They don’t present all options.”
And legally, they can turn a blind eye to the range of abortion options available to women with unplanned pregnancies.
The U.S. Supreme Court ruled in June 2018 that the crisis pregnancy centers were protected from California’s FACT Act, which built on already existing state laws regarding patients’ reproductive health privacy. The Act required licensed facilities to disseminate notice to all clients regarding California’s public programs that provide immediate, accessible, comprehensive family planning services including prenatal care and abortion. The Court ruled in favor of the crisis pregnancy center, assessing they were protected by the free speech clause of the First Amendment in NIFLA v. Becerra. Justice Clarence Thomas authored the majority opinion.
This ruling gave crisis pregnancy centers the green light to misrepresent their facilities to people in search of medical services, community resources, education, and materials that the pregnancy centers are rarely equipped to provide. In a concurrence, Justice Anthony Kennedy wrote:
The law is a paradigmatic example of the serious threat presented when government seeks to impose its own message in the place of individual speech, thought and expression.
Doctors in Arizona are not given that liberty.
Dr. Kwatra,
Arizona has already passed a bunch of laws that criminalize the practice of medicine, including criminalizing how we counsel our patients on abortion. It’s absolutely abhorrent.
Medical Fact Check SB 1164
In Arizona Nancy Barto, R-Phoenix sponsored SB 1164 and during committee hearings delivered her central messages in the solemn, slow tones of a graveside preacher.
Life is a human right.
State and medical standards place viability at 23 to 24 weeks. And the issue of viability isn’t just survival, it also means the capacity of very premature babies to thrive once they have left the neonatal unit. Only 1.3% of abortions in 2015 were performed after the 20th week of pregnancy and Arizona already prohibits the elective surgical termination of a fetus after 24 weeks.
During the Feb. 3 Senate Judiciary hearing on SB 1164, Gilbert Republican Sen. Warren Petersen and Barto argued the legislation would protect the emotional well-being of Arizona women.
Petersen,
Not only the physical, but perhaps the most dangerous is the mental. I have a dear friend who had an abortion. And not a day goes by that she does not need counseling. She still needs counseling.
Barto,
This law ensures that women are not put at risk at the greater risk of death and illness or psychological trauma, which later term abortions cause.

The American Psychological Association disagrees,
Women who are denied an abortion are more likely to initially experience higher levels of anxiety, lower life satisfaction and lower self-esteem compared with women who received an abortion. Experiencing unwanted pregnancies appears to be strongly associated with poor mental health effects for women later in life.
The racial component of the abortion debate, much like the delivery of healthcare services, was on the radar of legislators like Arizona Republican Rep. Walt Blackman.
One common chorus in Blackman’s argument was hard to believe and even harder to support.
Do you know there are more Black babies aborted than born?
Not in Arizona, where according to the Arizona Department of Health Services about 4,700 Black women gave birth in 2020 compared with about 1,600 Arizona women who elected an abortion. In Arizona about 12% of all abortions were performed on Black women, the 6th lowest in the nation, according to Kaiser Family Foundation.
Not in The United States, national abortion statistics from the CDC reveal 629,898 abortions were reported in the U.S. in 2019 with about 240,000 Black women choosing to end their pregnancies. More than twice as many (548,000) gave birth that year.
The state’s relentless pursuit to restrict abortion access, is what the people want, according to Barto,
US abortion laws allowing abortion up to birth, which is what Roe allows, are extreme and they’re out of touch with a large majority of Americans.
An extreme exaggeration according to a January 2022 Gallup Survey,
Americans’ satisfaction with the nation’s abortion laws is at a two-decade low of 24%. At the same time, the percentage saying they are dissatisfied because they think the laws should be less strict — broadly speaking, a “pro-choice” position on abortion — is at a new high of 30%. A smaller share of the population, 22%, is dissatisfied because they believe the laws should be stricter.
An even larger national poll from the Marquette Law School, also in January 2022,
Among those with an opinion on Roe, 28% say they are in favor of overturning the decision and 72% are opposed to overturning it.
When surveyed about a 15-week abortion ban, it’s more like a tie with 49% favoring the limitation on abortion, while 51% opposed it.
Barto’s global assessment of abortion rights was also repeatedly front and center of her remarks in support of her proposed abortion ban on Arizona women and physicians. She said,
America is only one among a handful of countries including North Korea and China that allow late term abortions.
There are 57 countries that offer abortion on demand, according to the World Health Organization’s Global Abortion Policies Database. According to a New York Times analysis, around a dozen countries allow abortions beyond 15 weeks of pregnancy. North Korea criminalizes abortion, with a penalty of up to three years imprisonment. China recently revised its abortion restrictions to curb the number of abortions for “non-medical reasons” due to concerns about declining population rates.
As for the current legislation’s lack of exceptions for rape or incest, Arizona will get attention for mirroring the Mississippi law now before the U.S. Supreme Court.
Most countries worldwide allow abortion in cases of rape and/or incest, either through exceptions or by permitting abortion on request.
As Barto and fellow Republicans in Arizona continue their push to limit or outlaw abortion, Barto will likely be front and center of the debate. As she said during House hearings in March,
If it were up to me, I think we would honor the life of a child born at conception.
No exceptions.
When signing into law SB 1164 March 30, Governor Ducey also signaled the fight wasn’t over, stating,
In Arizona we will continue to protect life to the greatest extent possible. In Arizona we know there is immeasurable value in every life – including preborn life.

Leave a Reply
You must be logged in to post a comment.